
Christianity and Depression, Tasia Scrutton
London : SCM Press, 2020
Tasia Scrutton’s ‘Christianity and Depression’ is an attempt to engage with the challenge of mental illness, specifically depression, from a broadly Christian point of view. She considers several different frameworks for understanding depression, such as depression being caused by individual sin, demonic possession, biological causation and so on. She also spends time on more metaphysical questions such as divine impassibility. The book is very good but somewhat uneven; in particular there is one significant omission in her treatment, which is very surprising given her explicit theological and political commitments.
In this review I will briefly outline her key points chapter by chapter before engaging in discussion.
Outline of chapters
In her introduction, Scrutton begins her work by articulating four caveats: that she is concerned with Christian understandings of depression; that concentrating on the interpretation and experience of depression is philosophically legitimate; that she will evaluate and assess the different Christian understandings giving a verdict on their worth; and finally that she will treat the various understandings as embodied in communal practices not just as individual belief-systems.
With respect to the definition of depression itself Scrutton chooses – very sensibly in my view – to consider as depression “anything that might reasonably be diagnosed as a depressive disorder by a doctor, whether or not the person has been to a doctor and been diagnosed”. She then clears further philosophical space by briefly addressing the hazards of a naïve dualism (mental vs physical) and the nature of what an illness is.
Scrutton’s first chapter is devoted to the idea that a person experiences depression as a result of sin in their life, that is, that the person has sinned and they experience depression as a consequence of their own sin. Scrutton rejects this understanding, on the grounds that it presupposes an incomplete understanding of human freedom; that it is in conflict with significant parts of the Christian tradition; and that it places unsustainable burdens upon those who are already vulnerable. In particular this approach deflects attention away from the social causes of depression in an individualistic manner.
The idea that depression is a result of demonic activity is the subject of Scrutton’s second chapter. Here she engages with the biblical record and integrates the exorcisms of Jesus into the wider inauguration of the Kingdom of God which was the principal characteristic of Jesus’ ministry. Again Scrutton largely rejects this framework for understanding depression, in particular on the grounds that “spiritual warfare should not be seen as an individual battle against the devil or some demons vying for our souls. These ideas have much more in common with element of contemporary US pop culture than they do with the gospel.”
For her third chapter Scrutton considers the idea that depression is an essentially biological problem like a broken leg or diabetes. In this chapter Scrutton argues straightforwardly for a ‘bio-psycho-social’ account of depression, which is a mainstream perspective within psychiatry that argues a) depression cannot be reduced to the biological but b) the biological is a necessary feature of clinical depression. Scrutton emphasises here that there is a rich Christian tradition that affirms our bodiliness, especially the fundamental doctrine of the resurrection of the body.
What is called ‘the dark night of the soul’ is the subject of Scrutton’s fourth chapter. Here the idea considered is that depression is something that is sent from God in order that the soul might grow closer to God through the experience of suffering, looking in particular at St John of the Cross. Scrutton argues that there is no direct correlation between depression and the dark night experience, and that it is important to keep the two concepts distinct.
Building from this, and starting to move away from interpretive frameworks, in chapter five Scrutton interrogates the idea that depression is something that can have a transformative effect upon the person experiencing it. Whilst the expectation of transformation can be oppressive, especially when that glides into the idea that the depression is not an evil as such, Scrutton supports the view that depression can be a redemptive process within which an evil can be transformed into a good, drawing in particular on the writings of Henri Nouwen to explain how.
I will take chapters six and seven together as they both deal with the issue of divine suffering (passibility). Chapter six is presented differently to the work as a whole, as an imagined dialogue between two guests on a radio show, one of whom believes in divine impassibility – the classical Christian position – and one of whom believes that ‘God suffers in Godself’, which is a view that has become more popular from the mid-twentieth century onwards. This chapter explores each view without taking a position. In the next chapter Scrutton considers whether the idea of a suffering God is actually helpful or consoling to those who suffer in this life, arguing that there is no advantage to the passibilist perspective in this respect and that, in particular, the way in which devotion to different saints happens in, eg, the Catholic tradition, enables an effective religious form of consolation for those who suffer.
Finally in her summary chapter Scrutton outlines her overall approach. Depression is not to be understood as the result of individual sin, nor as the consequence of spiritual attack by demons, nor as a gift from God given for spiritual growth but rather as a fruit of a disordered society: “If we wish to combat the root causes of depression, we need to think socially and politically about how our culture can enable people to live as communities and with sensitivity to the needs we have as human animals, rather than foster anxiety, loneliness and alienation”iv.
Discussion
I found Scrutton’s work to be philosophically rigorous and properly humble, in that she is explicit about her philosophical presuppositions and deductions. In writing clearly it becomes straightforward for a critic to engage and highlight differences. My principal objection is that Scrutton essentially reduces the phenomenon of human depression to being a product of an unjust social environment, effectively a social construction of depression. In contrast to this I would argue that depression is a phenomenon whereby multiple causes lead to similar outcomes and that the cardinal mistake to avoid is to conflate all the different experiences into a single form with a single cause.
So, for example, in the first chapter Scrutton argues against the view of depression as a result of sin committed by an individual, and that this presupposes an extreme voluntarism or exaltation of human freedom that is effectively Pelagian. I agree with much of this but would wish to insist that there are occasions when sinful choices lead to the experience of depression. Feelings of guilt and regret do in fact give rise to feelings of sadness, and if unaddressed that sadness can become malignant and meet the definition of depression that Scrutton depends upon. This does not invalidate the criticisms that Scrutton makes more generally, it is simply to insist that both the blanket allocation of depression to individual choice and the contrary blanket allocation of depression to social forces are equally in error. Much, perhaps most of depression in the West can be attributed to social contexts, but not all, and it seems that a fully Christian account of depression has to leave room for a form of depression that is the result of human sinfulness and rebellion against God.
Similarly, when considering demonic attack as a cause of depression Scrutton rightly draws together Jesus’ casting out of demons through exorcism with his wider proclamation of the Kingdom. Yet there are some significant gaps in her treatment of this issue, especially with regard to New Testament criticism. To begin with, Jesus’ proclamation of the Kingdom is bound up with a call to repentance, which can be both individual and corporate. Secondly, although Scrutton is correct to refer to the small number of exorcisms within Jesus’ ministry she does not address their programmatic nature and the way in which the evangelist treats them. So in Mark’s gospel the first action which Jesus takes is an exorcism and this is not an accident; rather this is the prototypical way in which Mark portrays Jesus as acting in power against the hostile spiritual forces of his time. This logic is taken to its conclusion with John’s gospel which does not contain an account of a personal exorcism but where the crucifixion itself is portrayed as having the character of an exorcism – “now is the Prince of this world cast out” (John 12.31). Thirdly, whilst correctly grounding this process of exorcism and spiritual warfare in the social context, Scrutton under-emphasises the importance of this to the wider New Testament writers such as Paul (see Walter Wink’s work). The language of principalities and powers, and the integration of the spiritual and the political that such language describes, is central to the Christian scheme of salvation. This is a surprising omission given how neatly it would fit with Scrutton’s overall approach.
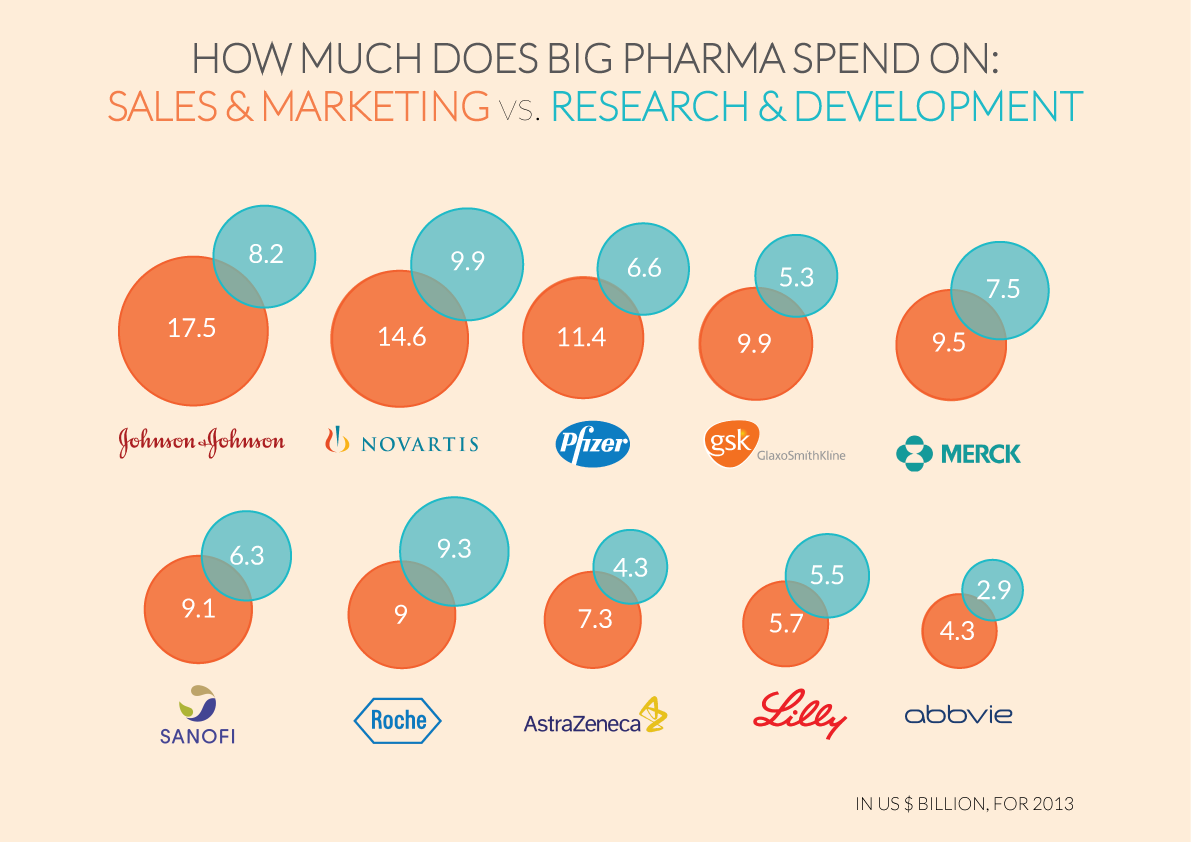
Which leads to my most fundamental criticism of Scrutton’s work which is the absence of any critique of the practice of contemporary psychiatric care, specifically the way in which the pharmaceutical companies act unethically. There is plentiful evidence (see Ben Goldacre’s Bad Pharma as a starting point) of the way in which, following the logic of industrial capitalism, pharmaceutical companies like Pfizer support the expansion of diagnostic criteria to include more and more human behaviours as ‘illnesses’ – which the companies can then develop treatments for in the form of patented drug therapies, through which they can generate continued profits. In addition to this the companies will systematically distort the scientific process in order to protect and increase their market shares. The social context that Scrutton rightly criticises as a principal factor causing depression cannot be understood without properly assessing the power that these actors bring to bear. These are in fact precisely the ‘principalities and powers’ that Christians need to be engaging with – and I see the absence of engagement with this as a missed opportunity on the part of Scrutton. I would wish to insist upon a properly Christian hermeneutic of suspicion in this context.
There remains much work to be done to develop a fully prophetic understanding of depression within the Christian tradition, but Scrutton has definitely moved the conversation forward and I would happily recommend the book to Christians interested in a deeper understanding of mental illness.





You must be logged in to post a comment.